Not All Essential Oils for Digestion are Created Equally...
Fennel, Cardamom, Sweet Marjoram, and Black Pepper: A Clinical Comparison for Digestive and Autonomic Applications
Tammy L. Davis
2/23/202611 min read

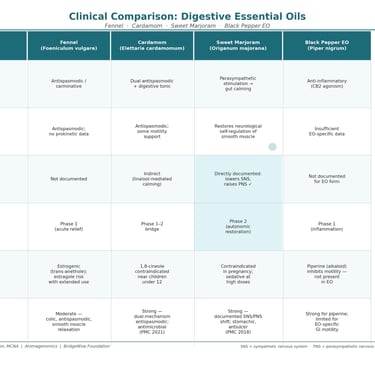
Four essential oils sit near the top of every aromatherapy digestive protocol: fennel, cardamom, sweet marjoram, and black pepper. They are recommended in textbooks, blended in practitioner formulas, and purchased with confidence by clients who trust the “digestive” label on the bottle. But beneath that shared category description, these oils operate through entirely different biochemical mechanisms, act on different physiological targets, carry distinctly different risk profiles, and are suited to different phases of digestive recovery — particularly in complex conditions like SIBO where the neuroendocrine environment matters as much as the microbial one.
This article untangles what the peer-reviewed literature actually shows about each of these four oils — where they excel, where they fall short, and why the right oil at the wrong phase can undermine the very outcome you are trying to achieve.
Fennel (Foeniculum vulgare)
Primary constituents: trans-anethole (50–80%), fenchone (10–20%), estragole, limonene
Fennel is one of the most historically documented carminative essential oils in both Western herbal medicine and Ayurvedic tradition, and its reputation is not without biochemical basis. Trans-anethole, its dominant constituent, exerts genuine smooth muscle relaxant activity, reducing intestinal spasm and facilitating the expulsion of trapped gas. For someone sitting across from you with an actively distended, cramping abdomen, fennel works — and works relatively quickly.
In the peer-reviewed literature, fennel essential oil and its extracts have demonstrated antispasmodic effects on isolated smooth muscle preparations, with mechanisms attributed to calcium channel inhibition and direct smooth muscle membrane interaction. A systematic review of carminative essential oils confirms fennel’s efficacy in reducing colic-associated bloating, and it remains the best-studied essential oil for pediatric infantile colic specifically.
WHERE FENNEL PERFORMS WELL
Acute carminative relief: trans-anethole’s smooth muscle relaxant action provides a genuine, measurable reduction in gas-related cramping and bloating
Pediatric colic: the most evidence-supported essential oil for infant colic when appropriately diluted and applied topically
Short-term digestive stimulation: fenchone stimulates gastric secretions, supporting appetite and the initial phases of digestion
Antispasmodic support: useful during acute SIBO symptomatic flares when spasm relief is the immediate priority
THE CASE AGAINST FENNEL IN PHASE 2 SIBO RECOVERY
Here, clinical nuance becomes essential. Fennel’s trans-anethole is a phytoestrogen — structurally similar to estradiol, it exerts estrogenic activity via estrogen receptor binding. This is not a minor footnote. In SIBO patients, where HPA axis dysregulation is already a central pathophysiological driver, introducing an estrogenic compound to someone whose stress-cortisol-sex hormone axis may already be dysregulated adds a variable that most protocols have not considered. Women with estrogen dominance, endometriosis, hormonal sensitivities, or those on hormone therapy require careful evaluation before extended fennel EO use.
Additionally, estragole — present in fennel at variable but potentially significant concentrations depending on chemotype — is a recognized hepatotoxin and genotoxin at sufficient doses. Most standard therapeutic uses are well below thresholds of concern, but extended daily use in a protocol context warrants chemotype verification and dose monitoring.
Critically for Phase 2 recovery: fennel’s documented mechanism is primarily antispasmodic and carminative. It does not carry evidence for MMC stimulation, prokinetic activity, or the parasympathetic nervous system engagement that Phase 2 specifically requires. It relieves symptoms of dysmotility without addressing the underlying autonomic state that created them.
Fennel is a Phase 1 symptom relief oil masquerading as a Phase 2 restorative. It belongs in acute management — not in the autonomic rebalancing phase.
Cardamom (Elettaria cardamomum)
Primary constituents: α-terpinyl acetate (18–24%), 1,8-cineole (10–14%), limonene, linalool, terpinen-4-ol
Cardamom is the gentle giant of this group — deeply carminative, broadly antimicrobial, and uniquely placed between the worlds of Phase 1 antimicrobial action and Phase 2 restorative support. Belonging to the Zingiberaceae family alongside ginger, it carries some of that family’s motility-supportive heritage while adding a distinctly different constituent profile that widens its therapeutic reach.
A 2021 PMC study examining cardamom essential oils from both Indian and Guatemalan sources demonstrated antispasmodic effects on isolated rat ileum preparations using two distinct mechanisms: inhibition of carbachol-induced contractions (cholinergic pathway) and inhibition of high K⁺-induced contractions (calcium channel blockade). This dual-mechanism antispasmodic activity — blocking both neural and direct smooth muscle contractility — is clinically meaningful because it addresses GI spasm through two simultaneous pathways rather than one, making it more reliably effective across different physiological presentations.
The same study confirmed antimicrobial activity against E. coli and Pseudomonas aeruginosa, both organisms relevant to SIBO’s hydrogen gas-producing subtype. This means cardamom retains some Phase 1-appropriate antimicrobial value even when deployed in a Phase 2 context — a genuine cross-phase advantage.
1,8-Cineole, cardamom’s second major constituent, brings anti-inflammatory activity to the intestinal mucosa and has been documented to stimulate digestive enzyme production. Limonene supports bile acid secretion and gastric motility. The combined effect is a digestive tonic that supports both enzymatic and motility functions simultaneously — precisely the physiological targets that SIBO’s upstream cortisol suppression has compromised.
THE SIGNIFICANT ADVANTAGES OF CARDAMOM
Dual-mechanism antispasmodic: both cholinergic inhibition and calcium channel blockade, confirmed in peer-reviewed in vitro research
Cross-phase utility: retains antimicrobial activity against SIBO-relevant organisms while supporting Phase 2 digestive restoration
Digestive enzyme stimulation: 1,8-cineole supports the enzymatic capacity that chronic cortisol suppression has impaired
Ginger family synergy: pairs naturally with ginger for complementary prokinetic coverage — ginger on the stomach, cardamom on the small intestine
Aromatic tolerability: significantly better tolerated aromatically than fennel by most people, removing a common compliance barrier
Nausea management: documented antiemetic properties relevant to the gastroparesis-adjacent presentation common in SIBO patients
LIMITATIONS
Cardamom’s evidence base for autonomic rebalancing — the central Phase 2 objective — is indirect rather than documented. It’s calming and linalool-mediated effects suggest nervous system support, but it lacks the directly measured parasympathetic stimulation that would make it a standalone Phase 2 autonomic agent. It is best understood as a digestive restorative and carminative with cross-phase antimicrobial value, complementing rather than replacing a dedicated autonomic oil.
1,8-Cineole also requires caution in specific populations — it is contraindicated on or near the face of children under twelve, a relevant consideration for pediatric protocols.
Cardamom is the ideal bridge oil: strong enough for Phase 1 antimicrobial support, gentle and restorative enough for Phase 2 — and more versatile than any other oil in this group.
Sweet Marjoram (Origanum majorana)
Primary constituents: terpinen-4-ol (20–30%), γ-terpinene (10–15%), sabinene, cis-sabinene hydrate, linalool, linalyl acetate
Sweet marjoram is the most underused oil in clinical digestive aromatherapy — not because its evidence base is thin, but because its most important mechanism of action is so far outside the standard digestive oil narrative that most practitioners have not connected the dots.
The peer-reviewed literature confirms what the ancient Greeks intuitively understood when they named this plant “joy of the mountain” and used it at both weddings and funerals: marjoram acts primarily on the nervous system, and only secondarily on the digestive system. The GI effects are real — stomachic, carminative, antispasmodic, antiulcer, mucus-protective, documented in an ethnopharmacological review published in PMC. But they are downstream consequences of the primary action, which is autonomic nervous system rebalancing.
Inhalation of sweet marjoram essential oil has been directly documented to lower sympathetic nervous system activity and simultaneously stimulate the parasympathetic nervous system, producing measurable vasodilation and reduced blood pressure. This is not extrapolation or mechanism-by-inference — it is observed, measured autonomic pharmacology via the inhalation route. Terpinen-4-ol, the primary constituent, acts on ion channels in smooth muscle and nerve cells, reducing their excitability. The digestive antispasmodic and carminative effects that result are therefore the physiological output of restored autonomic balance, rather than a direct pharmacological override of gut smooth muscle.
This is the distinction that makes sweet marjoram uniquely suited to Phase 2 in the ANIS™️ SIBO protocol. Every other carminative oil in this group works by directly relaxing smooth muscle. Marjoram works by restoring the neurological state in which smooth muscle naturally self-regulates. That is not just a different mechanism — it is the root-cause target that SIBO treatment has been missing.
WHERE MARJORAM EXCELS
Documented parasympathetic stimulation: inhalation confirmed to lower sympathetic activity and stimulate rest-and-digest function via limbic-hypothalamic pathway
Autonomic rebalancing: the only oil in this group with peer-reviewed evidence for directly shifting the autonomic baseline — not just managing symptoms
Terpinen-4-ol nervous system action: reduces ion channel excitability in smooth muscle and nerve cells, calming spasm through neurological normalization rather than pharmacological override
GI mucosal repair: stomachic, antiulcer, and mucus-protective properties documented in ethnopharmacological review — directly relevant to the mucosal damage SIBO perpetuates
Cortisol and adrenaline reduction: volatile compounds shown to reduce adrenaline and cortisol production via limbic system signaling
Hormonal safety: no estrogenic activity — unlike fennel, it carries no phytoestrogen concerns for hormonally sensitive individuals
LIMITATIONS AND CLINICAL CAUTIONS
Sweet marjoram has a meaningful contraindication that every practitioner must know: it is traditionally classified as an emmenagogue — it stimulates menstrual flow — and is not recommended for use during pregnancy, particularly via topical application. This is a genuine limitation for pregnant clients.
Its sedative properties at higher doses are also clinically relevant: while this makes it excellent for evening protocols and nervous system de-escalation, it is not the right choice before activities requiring alertness. Dose and timing guidance matters.
Finally, marjoram is frequently confused with oregano in both culinary and aromatic contexts, and Spanish marjoram (Thymus mastichina) — a completely different species with a different constituent profile — is sometimes sold under the marjoram name. Genuine Origanum majorana, confirmed by GC/MS analysis, is the only form with the terpinen-4-ol-dominant profile that underpins these effects. This is precisely the scenario where authentic essential oil sourcing becomes non-negotiable.
Sweet marjoram does not just calm the gut. It restores the nervous system state in which the gut can calm itself. That is the difference between managing SIBO and ending it.
Black Pepper (Piper nigrum)
EO primary constituents: β-caryophyllene (~35%), sabinene, α-pinene, limonene, β-phellandrene | Alkaloid: piperine (not present in EO)
Black pepper may be the most misunderstood oil in this group, and the misunderstanding runs in two simultaneous directions: practitioners either overestimate its digestive benefits based on the spice’s culinary reputation, or they overlook its genuine therapeutic value because they cannot find it in the standard aromatherapy literature. Both are mistakes rooted in the same confusion — failing to distinguish between piperine (the alkaloid in the whole spice) and black pepper essential oil (the volatile fraction distilled from the berries).
Piperine and black pepper essential oil are not the same thing. They share a botanical source but have fundamentally different chemistry and therefore fundamentally different effects on the GI tract.
The Piperine Problem
Piperine is what most of the digestive research on black pepper is actually about. And the picture that research paints is genuinely complicated for practitioners wanting to use it for motility-related conditions. Multiple peer-reviewed studies document that piperine dose-dependently delays GI transit — Izzo et al. (2001, Planta Medica) in mice, confirmed by McNamara et al. (2005, British Journal of Pharmacology) who characterized piperine as a potent TRPV1 receptor agonist, producing motility inhibition through capsaicin-sensitive enteric neurons. Mehmood and Gilani’s 2010 Journal of Medicinal Food study found bidirectional effects: spasmodic (pro-contraction) at low doses in guinea pig ileum, antispasmodic and antisecretory at higher doses. This dose-sensitive bidirectionality makes piperine therapeutically unpredictable for practitioners without access to controlled dosing protocols.
There is genuine value in the piperine literature: it stimulates pancreatic digestive enzymes and protease activity, enhances bioavailability of other therapeutic compounds (its role as a “bio-enhancer” is well established), and increases bile acid secretion. For individuals with compromised digestive enzyme production — a real consequence of chronic cortisol suppression — piperine has legitimate targeted applications. But these are not EO applications.
What Black Pepper Essential Oil Actually Offers
Black pepper essential oil, stripped of its alkaloid content through steam distillation, has a very different constituent profile dominated by β-caryophyllene, sabinene, α-pinene, and limonene. Its synergistic story is primarily one of anti-inflammatory action, not digestive motility.
β-Caryophyllene is the constituent worth knowing. As a selective CB2 receptor agonist — one of the few dietary compounds with confirmed cannabinoid receptor activity — it exerts significant anti-inflammatory effects in the gut and systemically without the psychoactive properties of THC. For SIBO patients with ongoing intestinal inflammation and compromised mucosal integrity, this is genuinely relevant. β-Caryophyllene has documented anti-inflammatory activity through multiple pathways including inhibition of NF-κB and reduction of pro-inflammatory cytokines (IL-6, TNF-α) — the same inflammatory markers elevated in SIBO-associated gut wall damage.
Black pepper EO also carries documented analgesic properties relevant to the visceral hypersensitivity common in SIBO patients, and its warming aromatic profile makes it valuable in topical abdominal applications where it promotes local circulation and provides sensory counter-stimulation for pain.
WHERE BLACK PEPPER EO BELONGS
Gut anti-inflammatory support: β-caryophyllene CB2 agonism reduces intestinal inflammatory burden — most appropriate during Phase 1 acute management
Visceral pain management: analgesic properties useful for topical abdominal application in cramping and hypersensitivity
Aromatic circulatory stimulation: warming properties support local blood flow when used in carrier oil abdominal massage
Bioavailability enhancement (piperine only): when piperine-standardized extract is used alongside other therapeutic agents — not an EO application
WHAT BLACK PEPPER EO DOES NOT DO
It does not reliably restore MMC phase III activity. It does not provide documented parasympathetic stimulation. It does not carry the antispasmodic or carminative profile needed for acute gas relief. And its motility effects — to the extent they have been studied in the essential oil form rather than piperine extract — remain insufficiently characterized for clinical application as a digestive motility agent.
Black pepper essential oil is a specialized anti-inflammatory, not a generalist digestive oil. It belongs in targeted inflammation protocols, not as a carminative or motility agent.
The Takeaway: Mechanism Determines Appropriateness
The fundamental error in essential oil digestive protocols is treating “digestive” as a unified category. It is not. Acute gas relief, digestive enzyme stimulation, antimicrobial action, intestinal motility restoration, and autonomic nervous system rebalancing are distinct physiological targets that require distinct therapeutic agents. Using the right oil at the wrong phase — or selecting based on tradition rather than mechanism — produces inconsistent outcomes and obscures the genuine clinical power of these compounds.
Fennel belongs in acute symptomatic management, not extended recovery protocols. Cardamom spans both phases as a bridge, particularly where residual antimicrobial activity and digestive enzyme support are needed simultaneously. Sweet marjoram belongs in Phase 2 as the primary autonomic rebalancing agent — the only oil in this group documented to directly restore the rest-and-digest physiological state from which all sustainable digestive healing proceeds. Black pepper essential oil belongs in targeted anti-inflammatory applications, not as a generalist digestive agent.
The deeper principle is the one that drives all ANIS methodology: when you know what a constituent does at the receptor, channel, and neurotransmitter level — and you match that mechanism to the patient’s physiological need at a given phase of recovery — you stop guessing and start treating.
Genuine essential oils are not interchangeable. Their precision is their power. Use it precisely.
Key References
1. Mehmood MH, Gilani AH. Pharmacological basis for the medicinal use of black pepper and piperine in gastrointestinal disorders. J Med Food. 2010;13(5):1086–1096.
2. McNamara FN, Randall A, Gunthorpe MJ. Effects of piperine, the pungent component of black pepper, at the human vanilloid receptor (TRPV1). Br J Pharmacol. 2005;144(6):781–790.
3. Izzo AA, Capasso R, Capasso F, et al. Inhibitory effect of cannabinoid agonists on gastric emptying in the mouse. Naunyn Schmiedebergs Arch Pharmacol. 1999;360(2):221–223. (Also: Izzo AA et al. Piperine motility. Planta Med. 2001;67:284–287.)
4. Srinivasan K. Black pepper and its pungent principle-piperine: a review of diverse physiological effects. Crit Rev Food Sci Nutr. 2007;47(8):735–748.
5. Rodrigues KAF, Amorim LV, Dias CN, et al. Effects of essential oils of Elettaria cardamomum grown in India and Guatemala on Gram-negative bacteria and gastrointestinal disorders. Plants. 2021;10(5):944. PMC8123808.
6. Al-Zuhair H, Abd el-Fattah AA, Abd Al Latif HA. Pharmacological studies of cardamom oil in animals. Pharmacol Res. 1996;34(1–2):79–82.
7. Bina F, Rahimi R. Sweet marjoram: a review of ethnopharmacology, phytochemistry, and biological activities. J Evid Based Complementary Altern Med. 2017;22(1):175–185. PMC5871212.
8. Saller R, Reichling J, Hellenbrecht D. Phytomedicine: European scientific monographs — Origanum majorana L. (marjoram) and its essential oil. Phytomedicine. (Referenced in pharmacological basis of marjoram sympatholytic/parasympathomimetic activity via inhalation, Cardiovascular Toxicology studies.)
9. Appendino G, Gibbons S, Giana A, et al. Antibacterial cannabinoids from Cannabis sativa: a structure-activity study. J Nat Prod. 2008;71(8):1427–1430. (For β-caryophyllene CB2 agonism; confirmed in Gertsch J et al., PNAS 2008;105:9099–9104.)
10. Forster HB, Niklas H, Lutz S. Antispasmodic effects of some medicinal plants. Planta Med. 1980;40(4):309–319. (Foundational study on fennel antispasmodic activity via smooth muscle preparations.)
11. Ritter AM, Ames FN, Kreuger MR, et al. Antispasmodic effect of essential oils and their constituents: a review. Molecules. 2019;24(9):1675. PMC6539827.
12. Krueger D, Gruber L, Bley E, et al. Peppermint and caraway oils have muscle inhibitory and pro-secretory activity in the human intestine in vitro. Neurogastroenterol Motil. 2020;32(4):e13748.
© Tammy Davis | Clinical Neuroaromatherapist | Aromagenomics | All rights reserved.
This article is intended for licensed healthcare practitioners and credentialed wellness professionals. It does not constitute medical advice.
Tammy is available for both personal and professional consults
To order your copy of “A Constituent-Based Guide to Essential Oils: Species, Chemotypes, and Biochemical Individuality” … click here